
Surgical Outcomes and Imaging
If you’ve been active long enough, you’ve likely hit a wall where Ibuprofen and "just resting it" stop cutting it. You get an MRI, you see words like "tear," "degeneration," or "thinning" in bold print, and suddenly the conversation shifts from your daily walks or gym sessions to a surgical consult. Regardless of your age or your sport, we tend to view surgery in one of two ways: it’s either the ultimate "fix" that will finally get you back to 100%, or it’s a sign that your most active years are behind you. In reality, neither is particularly accurate.
Anatomy vs. Capacity
The biggest misconception in modern orthopedics is that a "clean" image is the only way to have a high-performing body. You’ve likely been led to believe that if a piece of tissue is frayed or worn, it must be sewn back together or replaced to function. But at Summit Physio, we often see the gap between your anatomy (what you look like on a scan) and your capacity (how your body actually moves and handles load) every single day.
Often, the "pathology" found on your scan has been there for years, totally silent, while you were living your life and hitting your goals and is totally “normal”. The question you need to ask isn't just "What is torn?" but rather: "Is this finding actually the reason I’m hurting right now?"
Deciding whether or not to go under the knife is one of the most significant health decisions you’ll make. It shouldn’t be based on fear, a scary-sounding report, or a 10-minute conversation in a surgeon's office. It should be based on the numbers. In this blog, we will look at the actual success rates of the most common orthopedic procedures for the knee, shoulder, and back. We’ll compare the surgical outcomes to high-level conservative rehab so you can see where the evidence actually sits. Our goal is to help you move past the "broken" narrative and look at the statistics, so you can choose the path that actually gets you back to the life you love, not just the one that "cleans up" your MRI.
The MRI Trap: Why Your Scan Isn’t a "Broken" Warning
Before we look at the surgical data, we have to talk about the imaging report in your hand. MRI technology has become incredibly sophisticated. It’s so good, in fact, that it now picks up almost every "blemish" inside your body. The problem is that we’ve started treating these scans like a to-do list for a surgeon, when in reality, many of them are just the physiological cost of living an active life.
Think of someone who has spent their life working with their hands. Their palms are likely covered in calluses, scars, and thickened skin. If you took a high-resolution photo of their hands, you’d see a dozen "abnormalities." But those hands aren't broken, they’ve simply adapted and grown resilient over time. Your joints are exactly the same. Whether you are 25 or 75, we see a massive disconnect between what a scan shows and how you actually feel:
The Data: Structural Findings in Pain-Free Joints
The following statistics represent individuals who had zero pain and full function, yet underwent MRI imaging for research purposes. The results underscore just how common these "abnormalities" truly are.
Shoulder:
Seminal work by Yamamoto et al. (2011) and later systematic reviews by Barreto et al. (2019) fundamentally reshaped how clinicians interpret rotator cuff imaging. Yamamoto’s population-based study demonstrated that rotator cuff tears were present in more than 22 percent of the general population, the majority of whom had no shoulder pain and no loss of function. In other words, a substantial portion of people were unknowingly walking around with MRI-confirmed “tears” that had no clinical relevance.
Barreto’s review further reinforced this concept by showing a strong age-related increase in these findings. The prevalence of rotator cuff tears rose steadily with each decade of life, reaching rates as high as 50 percent in individuals over the age of 70, independent of symptoms. Importantly, these were not necessarily acute injuries or degenerative failures causing dysfunction. Rather, they appear to represent common age-related structural adaptations of tendon tissue.
Taken together, this body of research makes one thing clear: the presence of a rotator cuff tear on MRI does not inherently equate to pain, weakness, or impaired performance. Imaging findings must be interpreted in the context of the individual, their symptoms, their functional demands, and their physical examination. Without that context, structural “abnormalities” risk being overemphasized and incorrectly framed as the primary driver of pain or limitation.
Knee:
We often equate a “healthy” knee with a structurally pristine knee, assuming that the absence of pain must correlate with the absence of tissue changes. However, growing imaging research strongly challenges this assumption. A landmark study by Horga et al. (2020) sought to define what a truly “normal” knee looks like in real-world adults rather than idealized anatomy. Their cohort consisted of asymptomatic individuals with an average age of 44 years, all of whom reported no knee pain, no functional limitations, and no restrictions in daily or recreational activity.
Despite this, MRI findings were striking. An overwhelming 97 percent of participants demonstrated at least one structural “abnormality” on imaging. More than 30 percent had meniscal tears, and nearly 60 percent showed cartilage lesions. Importantly, these findings were not associated with pain, swelling, instability, or reduced activity levels. These individuals were functioning normally, often unaware that such changes even existed.
This challenges the traditional narrative that meniscal tears or cartilage defects are inherently pathological or symptomatic. Instead, the data suggest that these findings may represent common, age-related tissue adaptations rather than direct indicators of injury or dysfunction. Much like wrinkles in the skin or gray hair, structural changes within the knee appear to accumulate over time without necessarily compromising performance or quality of life.
The clinical implication is significant. When MRI findings are interpreted in isolation, there is a risk of attributing knee pain to structures that may be incidental and long-standing rather than causative. Pain, function, and tolerance to load cannot be reliably predicted by imaging alone. A meniscal tear or cartilage lesion on MRI does not automatically explain symptoms, nor does it mandate intervention. As with the shoulder, knee imaging must be contextualized within the individual’s history, physical examination, movement capacity, and response to load.
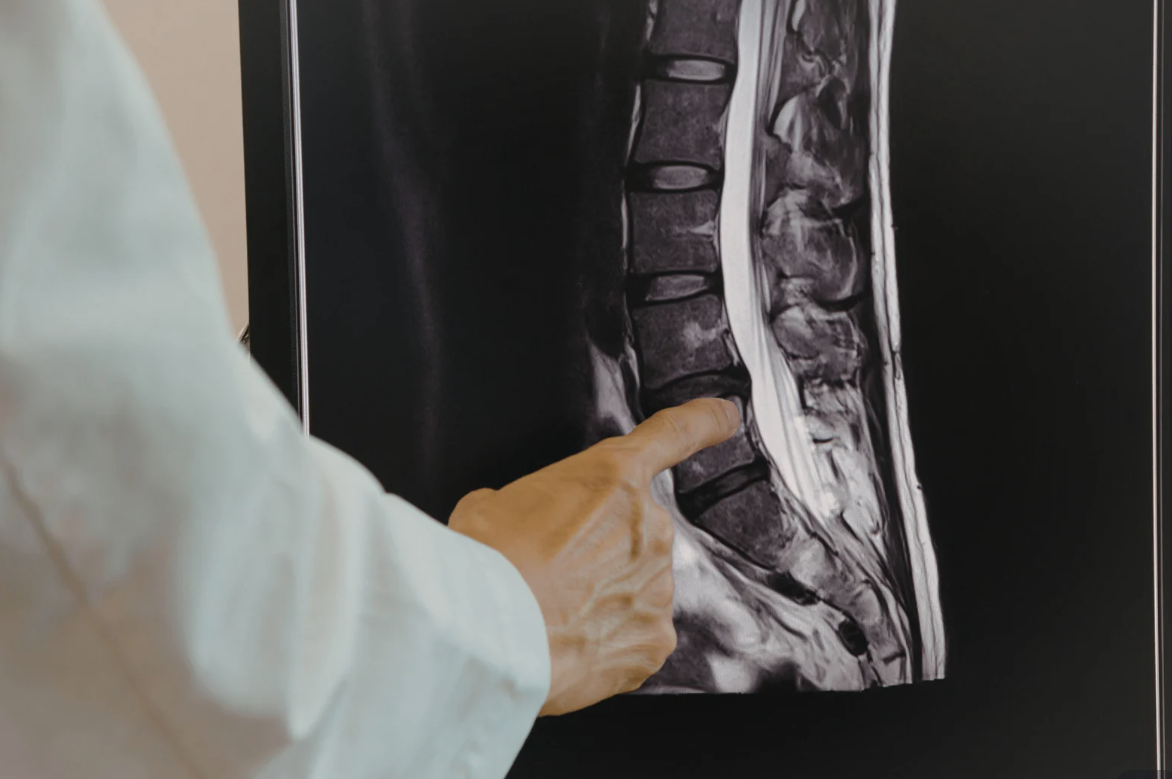
Spine:
Landmark research consistently shows that the spine is far more robust and adaptable than imaging reports often imply. Large-scale studies published in The Spine Journal and the American Journal of Neuroradiology have demonstrated that many findings commonly labeled as “degenerative” are, in fact, normal features of a living, aging spine rather than indicators of damage or failure.
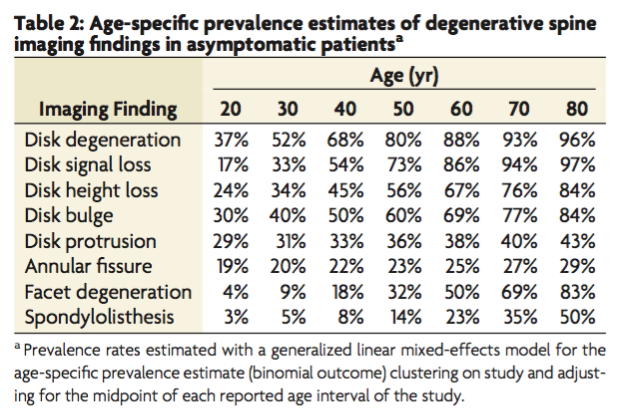
A major systematic review by Brinjikji et al. (2015) examined imaging results from over 3,000 asymptomatic individuals. The results were striking. By age 50, approximately 80 percent of pain-free people showed evidence of disc degeneration, and 60 percent had disc bulges. These individuals were living without back pain, functional limitation, or disability, yet their MRI reports would often read as anything but “normal.”
This pattern appears even earlier in life. Nakashima et al. (2015) studied more than 1,200 healthy volunteers and found that nearly 75 percent of people in their 20s already had disc bulges in the cervical spine despite having no symptoms whatsoever. These findings highlight that disc bulges are not inherently pathological and can exist long before pain ever enters the picture, if it does at all.
Beyond prevalence, imaging itself is not as objective as many assume. A revealing study by Herzog et al. (2017) demonstrated the variability of interpretation. One patient with back pain was sent to 10 different imaging centers, resulting in 49 total findings across reports. Not a single finding was identified consistently by all 10 radiologists. This underscores an uncomfortable truth: an imaging report reflects interpretation as much as anatomy.
Taken together, these studies reinforce a key point. Structural changes in the spine are common, expected, and often unrelated to pain. Imaging can provide useful information, but it cannot diagnose pain in isolation. Symptoms, movement tolerance, load capacity, and clinical presentation matter far more than what is written on a report.
To be clear, MRIs are a remarkable tool. If you’ve experienced significant trauma, if you’re dealing with "red flag" symptoms like progressive weakness or loss of sensation, or if you’ve given an honest go of conservative care (usually 12-16 weeks) without progress, a scan can be a vital piece of the puzzle. The goal isn't to avoid the MRI forever, we just want to ensure the scan is used to confirm a clinical suspicion rather than to dictate your entire recovery plan before you’ve even finished your first week of rehab.
A finding on your MRI is a valuable data point, but it should be the last thing we consider, not the first, when deciding if you are a candidate for surgery.
From Imaging to Outcomes: Does Surgery Deliver?
If your MRI isn't the whole story, the next question is simple: Will surgery get you back to 100% faster?
In the fitness community, we value being aggressive with our recovery. For years, surgery was marketed as the "fast track" to fixing the problem. However, when we look at the actual data comparing surgical intervention to progressive, performance-based loading, a surprising trend emerges. For many common procedures, the scalpel doesn't actually outperform a well-designed rehab program in the long run.
To make an informed choice, you have to look at the numbers. Let’s break down the actual success rates for the shoulder, knee and spine. .
Shoulder:

The Evidence
Many people are told they need a “clean up” surgery like subacromial decompression to fix shoulder impingement. But the research consistently shows surgery does not outperform physical therapy.
A large review by Nazari et al. (2019) found that adding surgery to rehab did not improve pain or function compared to physical therapy alone for shoulder impingement. Outcomes were essentially the same at both short- and long-term follow-ups. This is reinforced by Rutt et al. (2025) in Cureus, which compared arthroscopic subacromial decompression directly to physical therapy for Stage II shoulder impingement. Once again, no meaningful differences were found in pain, function, or return to daily activity between surgery and rehab.
The Verdict
Shaving bone or tissue to “create space” in the shoulder rarely delivers better results than rehab alone. Building strength, improving load tolerance, and restoring movement control is usually the more effective and lower-risk path for long-term shoulder health.
Knee:

The Evidence
Many people are told they need a "clean up" (meniscectomy) to stop their knee pain, but the data suggests that removing that tissue may actually be counterproductive. The OMEX Trial (Kise et al. 2016) compared surgery to exercise for degenerative meniscal tears and found no clinically relevant differences in pain or function at the 2-year mark.
This is reinforced by Skou et al. (2018) in JOSPT, which showed that exercise therapy provides similar pain relief to surgery but with far fewer long-term risks to joint health. Large-scale Cochrane Reviews (Arakgi et al.) have gone even further, showing that for degenerative knee disease, these "clean-up" surgeries rarely outperform a placebo or "sham" procedure where no tissue is actually removed.
The Verdict
Trimming a meniscus is often like shaving down a shock absorber to stop a squeak, it might help temporarily, but it leaves the joint with less protection. Strengthening your "suspension" (quads and glutes) is almost always the superior long-term play for both your performance and your joint longevity.
Spine:
The Evidence
Landmark research suggests that the body is much better at "self-healing" than we often give it credit for. Chiu et al. (2014) found that spontaneous regression of lumbar disc herniations occurs in roughly 66% of cases, meaning your immune system effectively resorbs the disc material over time. This is likely why Frogner et al. (2018) found that patients who see a physical therapist first for back pain have significantly lower long-term costs and are far less likely to end up in surgery or on long-term opioid prescriptions.
The Verdict
For the vast majority of disc-related pain, the "surgical" outcome is actually achieved by the body’s own natural healing process combined with progressive loading. Since imaging results can vary so widely between clinics, your recovery should be guided by your physical symptoms and progress, not just the words on a page.
The Surgical "Red Flags": When the Evidence Shifts
While the research strongly supports a "rehab-first" approach for most, there are specific clinical scenarios where the operating room becomes the most effective path forward. Generally, a surgical consult is prioritized when we see signs of neurological compromise or mechanical blockage. These may include:
Progressive Weakness: Loss of strength that is actively getting worse, such as "foot drop" or the inability to hold objects.
Neurological Changes: Loss of bowel or bladder control, or numbness in the "saddle" (groin) area.
Mechanical Locking: A joint that is physically stuck (usually the knee) and cannot be straightened, indicating a piece of tissue is physically blocking the movement.
Acute Traumatic Loss of Function: A sudden, high-force injury (like a fall or accident) followed by an immediate inability to move or load a limb and does not respond to therapy.
Failure to Progress: If you have committed to 12+ weeks of high-quality, performance-based physical therapy with zero improvement in your pain or ability to function.
Injections: In some cases, targeted injections may be considered to temporarily reduce pain or inflammation so meaningful rehab can occur. These are not a fix on their own, but a short-term tool to calm symptoms enough to tolerate loading, restore movement, and continue progress in physical therapy rather than replace it.
Every Case is Unique
It is vital to understand that the list above is not exhaustive. The human body doesn't always follow a textbook, and symptoms can manifest in ways that a bulleted list can't capture.
The Big Picture Takeaway: Capacity Over Anatomy




The evidence across the spine, knee, and shoulder is clear: your body is more resilient than a black-and-white MRI report suggests. Whether it’s a disc "self-cleaning" or a shoulder adapting to load, the research consistently shows that building capacity often outperforms altering anatomy.
However, while the data provides a powerful "birds-eye view" of success rates, it is vital to remember that you are not a statistic. Your training history, your specific goals, and how your body responds to load are variables that a research paper cannot capture. The "Red Flags" we’ve discussed are a vital safety net, but they aren't exhaustive. Every injury exists within the context of a unique human life, and some cases will always require a more nuanced, surgical approach.
Deciding how to handle a persistent injury shouldn't be based on fear or a 10-minute consultation. It requires a detailed look at how you move, how you've trained, and where you want to go. At Summit Physio, we help you bridge the gap between what your MRI says and what your body can actually do. If you are at a crossroads, let’s move past the "broken" narrative together. A professional, one-on-one evaluation with us is the only way to determine the best path forward for your specific goals.
Disclaimer: This post is for educational purposes and highlights current orthopedic literature; it is not a substitute for an individualized clinical exam. Because every case is unique, if you are considering surgery, you should be evaluated by us at Summit Physio & Performance or another qualified medical professional to discuss your specific clinical presentation and history.
Dr. Cat Cui, PT, DPT