
Ehlors-Danlos Syndrome: A Physical Therapy Perspective
Focus on Hypermobile Ehlors-Danlos Syndrome (hEDS)
Hypermobile Ehlers-Danlos Syndrome (hEDS) may sound rare, but new research suggests it could affect as many as 1 in 500 people, making it far more common than once believed and frequently missed or misunderstood. Many individuals live for years without answers, dealing with chronic pain, constant injuries, and unexplained fatigue. Patients have reported often being told everything is “normal.” In reality, studies show nearly 99% of people with hEDS experience persistent pain, along with common overlapping conditions like Postural Orthostatic Tachycardia Syndrome and Mast Cell Activation Syndrome. Despite this, diagnosis still relies on clinical recognition rather than a definitive test, leading to delays in answers that can stretch close to a decade. Understanding hEDS is the first step toward finally making sense of symptoms that many patients have been trying to explain for years, so let’s break it down!
What is Ehlers Danlos Syndrome?
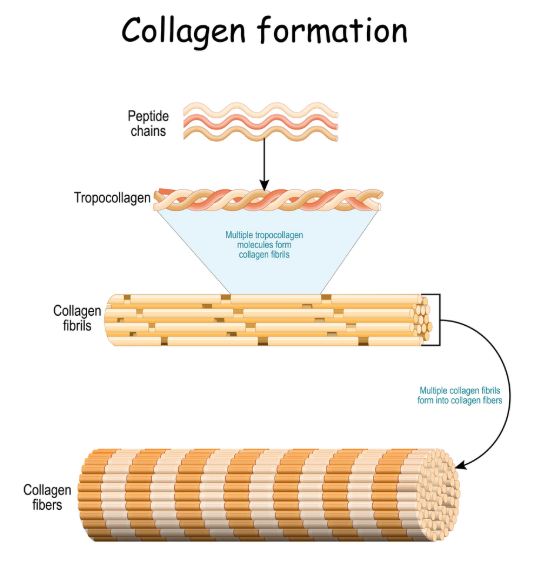
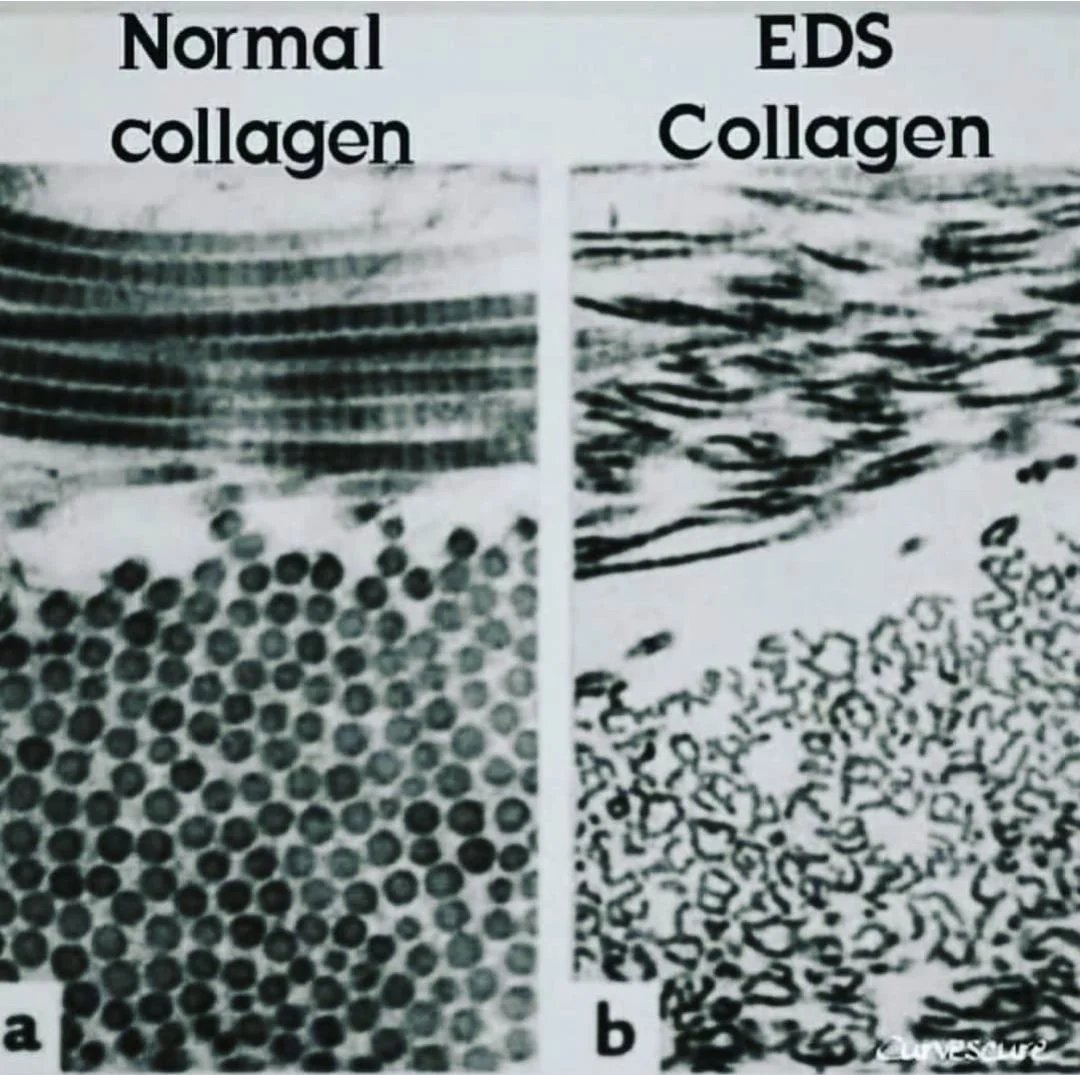
Ehlers-Danlos Syndrome (EDS) refers to a group of heritable connective tissue disorders caused by abnormalities in collagen structure, synthesis, or processing. Collagen is essential for the integrity of ligaments, tendons, skin, and other tissues, so dysfunction can affect multiple body systems.
The most recent classification (2017 International Classification of EDS) identifies 13 subtypes, each with distinct clinical and genetic features (Malfait et al., American Journal of Medical Genetics, 2017).
What Makes Hypermobile EDS Different?
hEDS is the most common type of EDS, accounting for about 90% of EDS cases. It it primary defined by:
Joint instability and frequent “giving out”
Recurrent sprains, subluxations, or dislocations
Chronic pain
Muscle fatigue and poor endurance
Delayed recovery from activity
Unlike other EDS subtypes, hEDS currently has no confirmed genetic marker, and diagnosis is based on clinical criteria (Malfait et al., 2017; Castori et al., American Journal of Medical Genetics, 2017).
Common Signs & Symptoms:
Patients with hEDS often present with
a combination of:
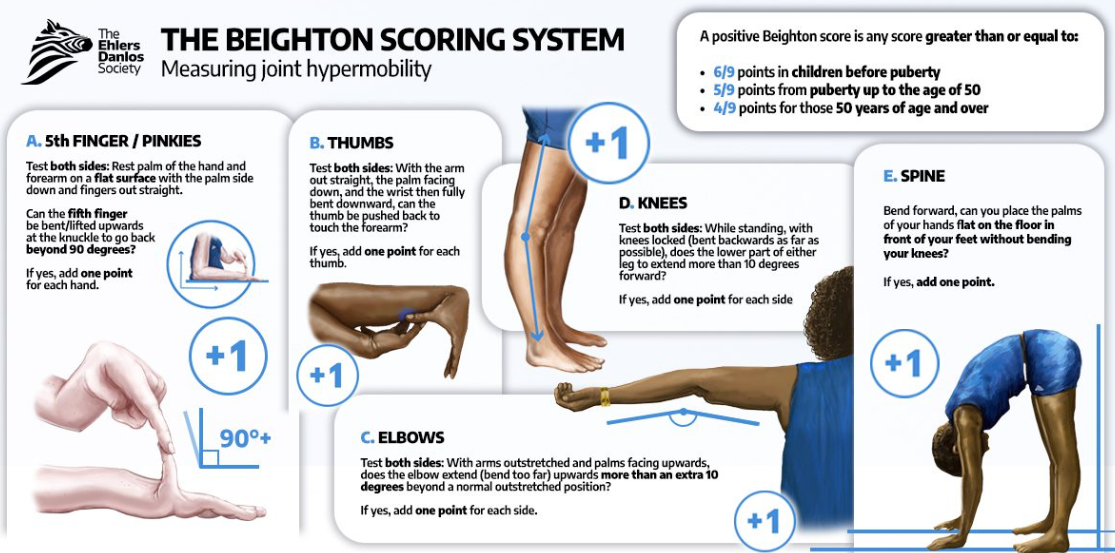
1. Joint Hypermobility & Instability
Increased joint range beyond normal limits
Ability to touch hands flat to the ground with straight knees
Ability to bend thumb backwards to forearm
Ability to perform the splits without training/effort
Higher risk of joint subluxations and dislocations
Ligamentous laxity leading to poor passive stability
2. Chronic Musculoskeletal Pain
Often begins in adolescence or early adulthood
Multifactorial: microtrauma, instability, central sensitization (nervous system being on high alert in response to pain)
Frequently persistent and widespread (Castori et al., 2017)
3. Proprioceptive Impairments
Reduced joint position sense
Altered neuromuscular control (Rombaut et al., Clinical Rheumatology, 2010)
4. Fatigue & Exercise Intolerance
Strongly reported across studies
Linked to autonomic dysfunction and deconditioning (Voermans et al., Seminars in Arthritis and Rheumatism, 2010)
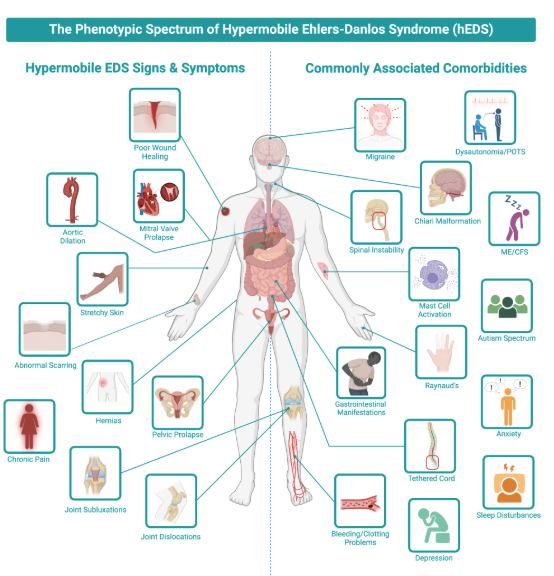
5. Associated Comorbidities
Postural Orthostatic Tachycardia Syndrome (POTS)
Gastrointestinal dysfunction
Mast Cell Activation Syndrome (MCAS)
Pelvic floor disorders
Headaches and cervical instability
Emerging literature continues to reinforce that hEDS is a multisystem condition, not purely musculoskeletal.
Why Physical Therapy Matters
Unfortunately, with this diagnosis, we do not have a magic fix or medication to cure all symptoms. There is strong consensus in the literature that conservative management, particularly physical therapy, is first-line treatment for hEDS (Engelbert et al., Pediatric Physical Therapy, 2017; Palmer et al., Disability and Rehabilitation, 2020).
However, outcomes depend heavily on appropriate programming. Meaning, there is not a one size fits all approach or protocol to this diagnosis.
Traditional approaches that focus heavily on stretching or aggressive strengthening can sometimes worsen symptoms. Instead, PT for hEDS should emphasize:
1. Prioritize Stability Over Mobility
Patients with hEDS already have an excessive range of motion.
Studies emphasize strengthening within controlled ranges, not increasing flexibility.
2. Target Proprioception & Neuromuscular Control
Impaired sense of body in space is well documented
Balance training and motor control exercises improve joint stability and function
3. Use Low-Load, Progressive Strengthening
Gradual resistance training improves function without exacerbating symptoms
Isometric and closed-chain exercises are commonly recommended
4. Address Overactive Nervous System & Pain
Chronic pain in hEDS is not purely structural
Incorporating pain neuroscience education improves outcomes (Baeza-Velasco et al., Rheumatology International, 2018)
5. Incorporate Fatigue & Autonomic Management
Pacing strategies are critical
Exercise programs should be graded and individualized
Additionally, newer systematic reviews show that conservative interventions (exercise, stabilization, education) can improve pain, function, and quality of life, although high-quality trials remain limited. Therefore, consistency is key. Progress may be slower, but the goal is sustainable function, not quick fixes.
Common Mistakes to Avoid
Overstretching: Often worsens instability
Pushing through pain: Can lead to flare-ups
High-impact training too soon: Increases injury risk
Ignoring fatigue: Leads to setbacks
New Research
Emerging research suggests that hEDS may be more than just a connective tissue disorder, it may also involve the immune system. Recent studies analyzing nearly 4,000 patients found that hEDS affects the whole body, with many individuals reporting joint instability/pain (up to 99%), digestive issues, and nervous system dysfunction. Researchers have also identified potential genetic links and changes in blood proteins related to inflammation, immune response, and clotting, helping explain why symptoms can flare or feel unpredictable.
This newer understanding is just a snapshot of ideas they are exploring, but it better matches what patients have been saying for years: hEDS is not just about “loose joints,” but a complex, multisystem condition that may involve the connection between the immune system, nervous system, and gut. While this research is still evolving, it opens the door for earlier diagnosis and more targeted treatments in the future.
Recommendations
Primary Care Providers in Colorado Springs
Gorman Medical Clinic
Specializes in connective tissue disorders, pain management, hormone therapy
Additional Resources
The Ehlors-Danlos Society
Why Genetic Testing is Important - https://www.ehlers-danlos.com/resource/genetic-testing-for-eds-why-we-do-it-why-it-matters/
In Conclusion
hEDS is often underdiagnosed or misunderstood, with many patients experiencing delayed diagnosis and fragmented care. Literature highlights the importance of a multidisciplinary approach and individualized care for each case. Early guidance helps you avoid common setbacks and builds a plan that actually works for your body, not against it.
Hypermobile EDS requires a shift in how we approach rehabilitation. Evidence supports that:
Physical therapy is essential but must be individualized and strategic
Stability, motor control, and pacing are key drivers of success
Long-term outcomes depend on consistency, not intensity
For patients, the goal is not to eliminate hypermobility, but to build resilience, improve function, and reduce symptom burden over time.
Dr. Bree Martin, PT, DPT, hEDS Specialist
FAQs about Ehlors-Danlos Syndrome
1. What are the early signs of Hypermobile Ehlers-Danlos Syndrome (hEDS)?
Common early signs of Hypermobile Ehlers-Danlos Syndrome include frequent sprains, joints that “give out,” chronic joint or muscle pain, extreme flexibility, fatigue, and slow recovery after activity. Many people also report dizziness when standing, digestive issues, or headaches.
2. Can physical therapy help with Ehlers-Danlos Syndrome?
Yes. Physical therapy is considered first-line treatment for Ehlers-Danlos Syndrome. The key is working with a provider who understands that treatment should focus on building joint stability, improving body awareness (proprioception), and gradually strengthening without overstretching already flexible joints.
3. Why does it take so long to get diagnosed with hEDS?
There is currently no single blood test or genetic test to confirm hEDS. Diagnosis is based on clinical criteria and symptom history, which means many people are misdiagnosed or told their symptoms are “normal” for years before getting answers.
4. Where can I go for hEDS treatment?
Finding a provider who understands Hypermobile Ehlers-Danlos Syndrome (hEDS) is key to effective care. Physical therapy with a clinician experienced in hypermobility can help improve joint stability, reduce pain, and build long-term strength safely.
Fun fact: Our own Dr. Bree Martin specializes in working with individuals with hEDS and has advanced training in treating this condition.
References
Malfait F, Francomano C, Byers P, et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):8-26. doi:10.1002/ajmg.c.31552
Castori M, Tinkle B, Levy H, et al. A framework for the classification of joint hypermobility and related conditions. Am J Med Genet C Semin Med Genet. 2017;175(1):148-157. doi:10.1002/ajmg.c.31539
Rombaut L, Malfait F, De Wandele I, et al. Muscle-tendon tissue properties in the hypermobility type of Ehlers-Danlos syndrome. Arthritis Care Res (Hoboken). 2012;64(5):766-772. doi:10.1002/acr.21592
Voermans NC, Knoop H, Bleijenberg G, et al. Fatigue is a frequent and clinically relevant problem in Ehlers-Danlos syndrome. Semin Arthritis Rheum. 2010;40(3):267-274. doi:10.1016/j.semarthrit.2009.06.004
Pezaro S, et al. Management of childbearing with hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorders: a scoping review. PLoS One. 2024.
Brittain MG, Flanagan S, Foreman L, Teran-Wodzinski P. Physical therapy interventions in generalized hypermobility spectrum disorder and hypermobile Ehlers-Danlos syndrome: a scoping review. Disabil Rehabil. 2024;46(10):1936-1953. doi:10.1080/09638288.2023.2216028
Higo A, Palmer S, Liaghat B, et al. The effectiveness of conservative interventions on pain, function, and quality of life in adults with hypermobile Ehlers-Danlos syndrome: a systematic review. Arch Rehabil Res Clin Transl. 2024;6(3):100360. doi:10.1016/j.arrct.2024.100360
Buryk-Iggers S, Mittal N, Santa Mina D, et al. Exercise and rehabilitation in people with Ehlers-Danlos syndrome: a systematic review. Arch Rehabil Res Clin Transl. 2022;4(2):100189. doi:10.1016/j.arrct.2022.100189
Tudini F, Jordon M, Levine D, et al. Effects of kinesiology taping on shoulder range of motion and proprioception in hypermobile Ehlers-Danlos syndrome: a randomized controlled trial. Front Rehabil Sci. 2024. doi:10.3389/fresc.2024.1383551
Daylor V, Griggs M, Weintraub A, et al; Norris RA. Defining the chronic complexities of hypermobile Ehlers-Danlos Syndrome and hypermobility spectrum disorders: a global survey of diagnostic challenges, lifelong comorbidities, and unmet needs. J Clin Med. 2025;14(16):5636. doi:10.3390/jcm14165636
Gensemer C, Petrucci T, Beck T, et al; Norris RA. KLK15 alters connective tissues in hypermobile Ehlers-Danlos Syndrome. iScience. 2025;28(9):113343. Published August 12, 2025. doi:10.1016/j.isci.2025.113343
Griggs M, Daylor V, Petrucci T, et al; Norris RA, Gensemer C. Immune dysregulation and proteomic alterations in hypermobile Ehlers-Danlos Syndrome. ImmunoHorizons. 2025;9(10):vlaf044. doi:10.1093/immhor/vlaf044